
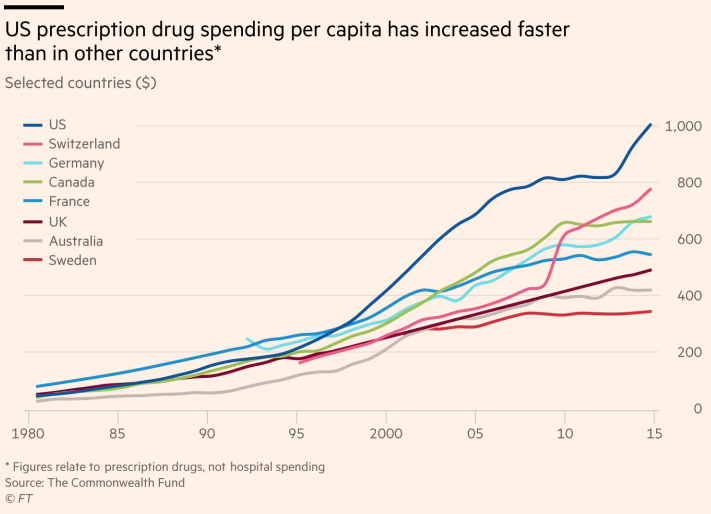
Americans are paying approximately 2.5 times as much as other developed countries for identical drugs, and high prices are leading some individuals to forego, modify, or delay treatments – leading to loss of life. The issue is seemingly a no-brainer politically, with Republican and Democratic majorities supporting allowing the federal government to negotiate prescription drug prices, but change has been slow to come. Promises that former president Trump was making back in 2018 (“You’ll be seeing drug prices falling very substantially in the not-too-distant future, and it’s going to be beautiful”) look very similar to ones President Biden is making today (“I’m committed to using every tool I have to lower prescription drug costs for Americans”). So, why are drug prices so high, and what can be done about it?
Factors Contributing to High Drug Prices in the U.S.
The U.S. approval process for new drugs is designed to reward innovation. After the U.S. Food and Drug Administration (FDA) approves a new drug as fit for human consumption, the patenting company enjoys exclusive rights to the drug. This means that for a period of time, usually upwards of 20 years, the manufacturer holds a monopoly on this specific drug and can therefore profit handsomely from their innovation and effort. As drug companies frequently highlight, the cost of developing new drugs is highly expensive and fraught with failure; the industry is high risk, and exclusivity means it is also high reward. While this approach rightfully rewards innovation, it also has some major issues, several of which are detailed below.
Lack of Oversight: Unlike in some other developed countries, there is no mechanism through which the U.S. government can regulate prices, which leaves drug companies the ability to essentially charge as much as they want or as much as they think the market can support. This means drugs can easily be priced out of a manageable range for certain patients.
Please check your email for instructions to ensure that the newsletter arrives in your inbox tomorrow.
Monopoly: New medications often have no alternatives, meaning consumers are stuck paying whatever price the patenting company decides, regardless of whether that cost is proportional to the actual benefit offered by the drug. Additionally, “for serious diseases, patients and their families are willing to pay any price in order to save or prolong life.”
Patent Manipulation: Nominally, the system is supposed to temper high prices through the introduction of generic replacements following the period of exclusivity granted by the initial patent. However, drug companies often manipulate the use of patents to their advantage in several ways:
- Evergreening: In this process, pharmaceutical companies make minor alterations to existing drugs that are sufficient enough to secure a new patent, even if the actual efficacy of the drug is unchanged. (Remember, the FDA’s job is to assess whether a drug is fit for human consumption, not if it is effective. As long as a drug achieves FDA approval for safety, companies can charge, and advertise for the drug, however much they want.)
- Patent thickets: Companies engineer complex tangles of intellectual property rights, often involving subcomponents of the drug in question, to deter competition.
- “Pay for delay” agreements: Drug companies may even go as far as to pay off competitors to delay introducing generic alternatives for a certain drug into the market.
- Planned obsolescence: Rapid advancements in medical knowledge mean medicines often become obsolete before the initial patent runs out.
In effect, the design of the current system means consumers may never enjoy lower-cost drugs but instead are stuck in a cycle of paying a premium. It’s also how Martin Shkreli, the infamous “pharma bro,” raised the price of a decades-old anti-parasitic drug from $13.50 a pill to $750. Shkreli’s company was able to upcharge so much because it “created ‘a web of anticompetitive restrictions’ to prevent other companies from creating cheaper generic versions.”
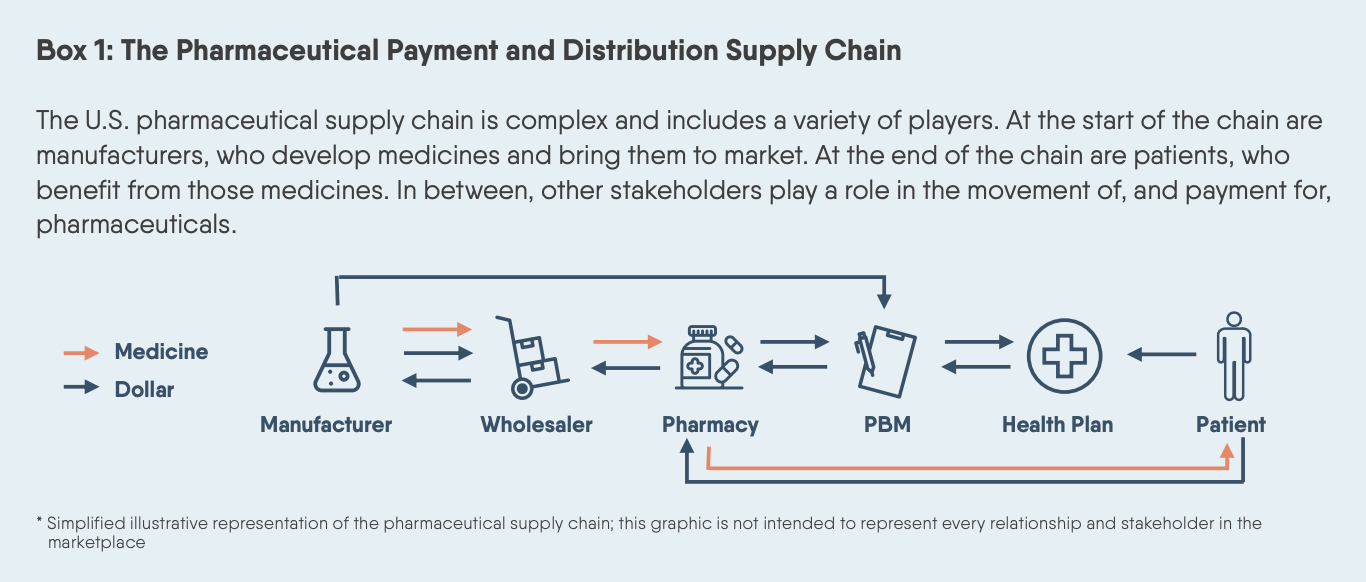
Lack of Negotiating Power: The marketplace for drugs is hindered at a larger, structural level by the bespoke nature of price negotiations. Whereas drug companies in other countries such as the United Kingdom and France negotiate drug prices with the government, drug companies in the U.S. engage with health providers, insurance companies, and government agencies on a case-by-case basis, often with significant opacity. Two important examples of this issue are pharmacy benefit managers (PBMs) and Medicare’s inability to negotiate prices.
- PBMs: PBMs are intermediary companies that “use complex business models to manage prescription drug program services for employers and health care insurance companies,” including rebates from manufacturers and discounts for retail pharmacies. However, PBMs have been strongly criticized for a range of opaque practices that maximize their profit, withhold savings from consumers, and interfere with the effective treatment of patients. Overall, the details of more than 40% of PBM revenue cannot be calculated.
- Medicare: The Medicare Modernization Act of 2003 forbids Medicare from negotiating drug prices at all, meaning Medicare is a captive market. Since the law was put in place, drug companies have even targeted medications covered by Medicare for R&D, sacrificing innovation elsewhere for guaranteed high profits. (For comparison, the Department of Veterans Affairs is allowed to negotiate prices and pays roughly 40% less than Medicare for the same drugs.)
The Problems with Pharmacy Benefit Managers
Pharmacy benefit managers (PBMs) claim to be key advocates for consumers, securing lower prices for drugs, reducing waste, and improving care. The Pharmaceutical Care Management Association — the industry’s trade association — estimates PBM’s will produce cost savings of $654 billion between 2016 and 2025. However, PBMs are commonly targeted as one of the most problematic segments of the drug supply chain.
PBMs negotiate rebates from drug manufacturers, which are ostensibly passed down through the supply chain through pharmacies and health insurers to ultimately benefit consumers. In reality, however, PBMs are under fire for a range of practices that maximize their own profit at the cost of consumers. Practices such as “step therapy” and “non-medical switching” see PBM’s make patients try alternative drugs with higher profit margins than what they were prescribed, often with medical consequences. And PBMs may even fail to pass on savings down the drug supply chain. Under “spread pricing,” PBMs may charge a payer more than they reimburse to the pharmacy, and then pocket the difference.
In aggregate, the current system leaves consumers paying higher prices than the rest of the world. These high costs are having huge impacts. People are delaying treatment for curable illnesses, rationing medications and suffering the side effects, traveling vast distances to procure medication elsewhere, or are simply facing death, priced out of securing the medication they need to survive.
Can Government Oversight Solve High Drug Prices?
For some, the solution is obvious: the government needs to step in with regulation to deter some of these practices. Advocates of increased oversight argue that a government body could (1) help determine costs that are accessible to consumers but that also still provide ample profit to the producer, (2) ensure that “new” drugs actually deliver additional benefits justified by the price, and (3) deter practices like “evergreening” and allow lower-cost options to reach the market more frequently.
A key part of this approach is the establishment of value-based pricing, meaning that medications are, to an extent, priced in relation to their actual value to customers. Certain medications are heavily marketed and pushed by pharmaceutical companies without actually delivering any demonstrated additional benefit vis-à-vis pre-existing options. For example, drug companies are keeping the cost of insulin high or raising it further by developing new formulas that, while technically patentable, may not actually offer any additional benefit to most diabetics. An oversight body could help set prices proportional to a medication’s actual benefit and ensure that patients aren’t priced out of the drugs they need to be healthy.
The Soaring Cost of Insulin
The poster child of high drug prices is insulin, a life-saving treatment for the 1 in 10 Americans who have diabetes. The drug was discovered over a century ago, and the rights were sold to the University of Toronto for $1, with the inventor citing the ethical issues of profiting off of a discovery that could save lives. Today, the drug has largely been monopolized in the U.S. by three companies — NovoNordisk, Sanofi-Aventis, and Eli Lilly — which continue to charge steep prices through evergreen patents and a lack of regulatory oversight. As a result, the cost of insulin has risen far faster than inflation since the 1990s. In 1999, a vial of Humalog (insulin lispro) cost $21; 20 years later, it cost $332.
At the same time, there is no shortage of opposition to increased government oversight. Pharmaceutical companies argue that advancements in medicine are in part due to the free market incentives that attract investment toward high-risk, high-reward endeavors that make it desirable to take risks to develop new drugs. Drug companies also suggest that much of these profits are reinvested into new R&D endeavors, without which the drug industry may not be as effective. As Kenneth Fraizer, the CEO of Merck, put it, “What keeps me up [at night] . . . is the concern that we will not have a viable, predictable market that will allow people to continue to put the very large amounts of money up at risk for a very long period of time, in an attempt to find solutions to some of the hardest problems like Alzheimer’s.”
Please check your email for instructions to ensure that the newsletter arrives in your inbox tomorrow.
The numbers show that pharmaceutical companies are as profit-driven as other industries and that profits are not necessarily prioritized for new R&D. For example, 14 large pharmaceutical companies spent $577 billion on stock buybacks and dividends between 2016 and 2020, $56 billion more than what they spent on R&D. According to the Financial Times, “major pharma companies make about twice as much in profit each quarter as they spend on R&D,” and most companies spend a significantly larger sum on sales and marketing. As the Center for American Progress put it, “there is not a significant relationship between the prices charged by pharmaceutical companies and either their research and development (R&D) spending or the clinical benefit of their products.” Conclusions like these feed into the perception that the process for developing new drugs, at least to some degree, works more in favor of drug companies and their investors than the patients who need effective and affordable healthcare.
The Gridlocked Search for Solutions
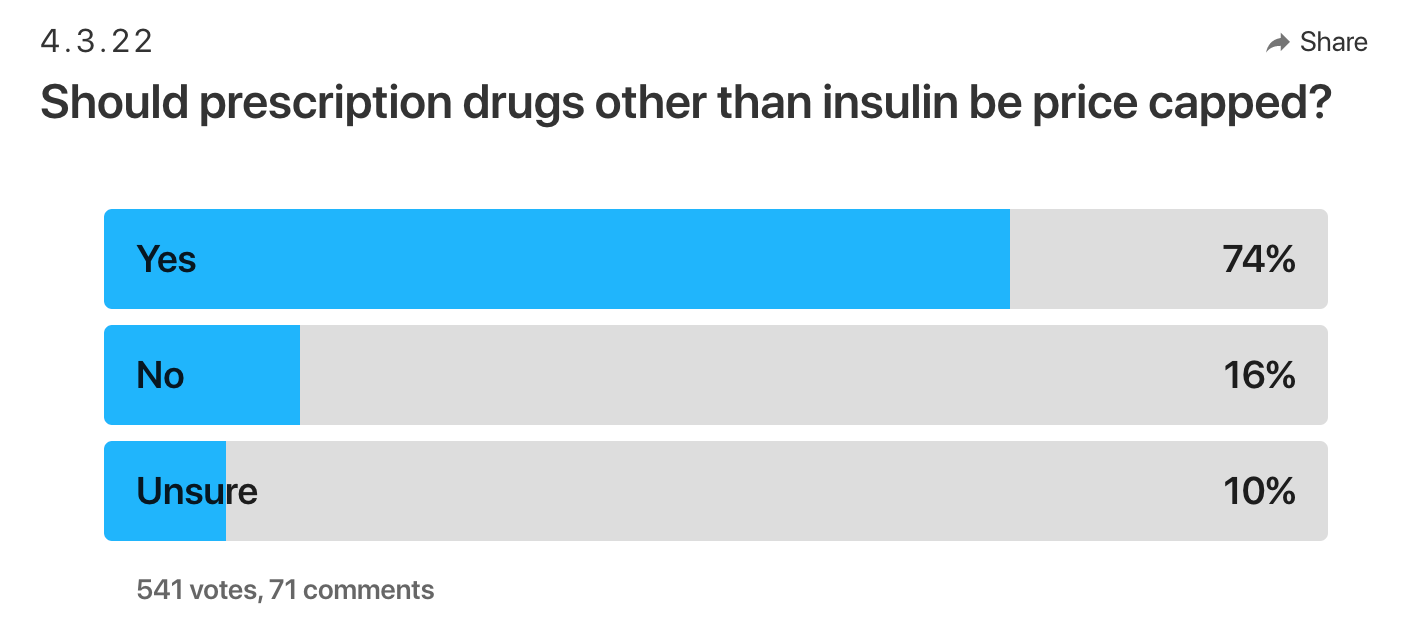
One thing is clear: Americans strongly support lowering drug prices. As the Kaiser Family Foundation notes: “Large majorities supported the idea of Medicare negotiating with pharmaceutical firms to get lower prices for both its beneficiaries and people with private insurance: 83% overall, including 95% of Democrats, 82% of independents and 71% of Republicans.” So, why hasn’t change already happened?
Even if everyday citizens largely agree that government action needs to be taken, Republican and Democratic politicians disagree on what those steps should be. Republican politicians broadly disagree with setting price caps, reflecting the worry that regulation will infringe upon the incentives that drive innovation and investment in the industry. Instead, they have favored making it easier to get more competing drugs to the market, including generic alternatives, and easing the regulatory burdens imposed by the FDA. Democratic politicians, by contrast, generally support a larger role for government in the pharmaceutical industry and favor immediate relief to consumers through legislation. It’s worth remembering, however, that as much as two-thirds of Congress cashed a campaign check from the pharmaceutical industry in 2020, which is likely slowing the pace of legislative action.
This disagreement means that proposed fixes for the issue have a dim outlook. Provisions in the stagnant Build Back Better bill would allow Medicare to negotiate drug prices, cap co-pays for drugs in some circumstances, penalize drug companies that raise drug prices faster than inflation, and implement targeted measures on some of the most problematic drugs (e.g., insulin) to keep costs down for consumers. With this major legislation package stalled, the House recently passed the Affordable Insulin Now Act, which would cap insulin prices at $35 a month or 25% of an insurance plan’s negotiated price, whichever is lower. Though the bill passed the House with 220 Democrats and 12 Republicans, making it somewhat bipartisan, it is unlikely to receive sufficient Republican support to pass in the Senate.
Tired of waiting, some in the private sector are looking to drum up solutions of their own. Civica Rx is a non-profit company focusing on producing low-cost generic drugs. Their goal is to partner with healthcare systems to make generic drugs affordable and available, which includes an effort to lower the price for insulin by as much as 80%. As another example, billionaire entrepreneur Mark Cuban, a recent guest on The Factual’s Unbiased podcast, has launched the Cost Plus Drug Company, an online pharmacy that promises to cut out the middlemen and pass savings on to consumers. Such efforts are a start, but they can do little to influence the market of drugs that fall under patents.
For real change, Republicans and Democrats need to pass legislation that more thoroughly addresses the system as a whole. Such an effort will likely involve multiple policies favored on either side, including revised patent schemes, increased competition, lower barriers to market entry, and maybe even price caps. Until then, Americans are set to keep paying a premium for medications.